Orthopedic Surgery: Overview Of Common Procedures And Care Pathways
Types of Procedures and Indications within Orthopedic Surgery
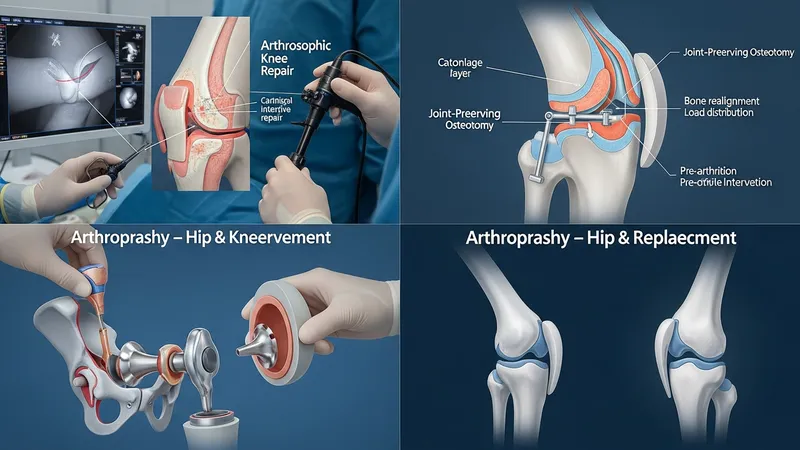
Procedural selection in orthopedic practice generally follows anatomic diagnosis, symptom burden, and functional limitation. Joint-preserving procedures such as osteotomy or cartilage repair may be considered when degenerative changes are limited and the goal is to maintain native joint structures. Joint replacement (arthroplasty) is often considered when articular surfaces are extensively compromised and pain or function is substantially affected. Fracture fixation choices depend on fracture classification, bone quality, and soft-tissue status, with options ranging from internal plates and screws to intramedullary nails and external fixators. Indication patterns may vary by age, activity level, and comorbidity profile.
Minimally invasive arthroscopic techniques are frequently applied to intra-articular pathology because they can allow targeted repair through small incisions and may reduce soft-tissue disruption. These methods often address meniscal tears, ligament injuries, or chondral lesions using specialized instruments and suture-based repairs. Conversely, open procedures remain necessary for extensive reconstructions, complex fracture patterns, or when direct exposure is required for stable fixation. Decision-making commonly weighs the anticipated tissue environment, repair durability, and rehabilitation implications rather than assuming one approach fits all cases.
Implant and fixation technology choices can substantially influence operative planning and postoperative management. Implant options include cemented versus cementless components in arthroplasty, modular designs for complex reconstructions, and a variety of plate and nail systems for fractures. Material properties, biomechanical fit, and surgeon familiarity typically inform selection. In many clinical settings, implant registries or institutional protocols may provide comparative data on performance patterns, which can help practitioners align device choices with expected operative scenarios while acknowledging that outcomes depend on multiple interacting factors.
Indication thresholds and timing for surgery also reflect broader care pathway goals, including optimization of health status before intervention. For elective procedures, preoperative optimization of nutritional status, glycemic control, or cardiovascular risk factors may be integrated into the pathway to reduce perioperative variability. For acute injuries, timing decisions often balance the need for early stabilization with the requirement to address soft-tissue concerns. These considerations typically aim to create a predictable operative environment and a structured rehabilitation trajectory.