All-on-4 Dental Implants: Understanding The Full-Arch Restoration Procedure
Surgical Steps and Implant Placement Considerations for Four-Implant Full-Arch Restorations
Surgical sequencing commonly starts with atraumatic extractions when necessary, followed by alveolar debridement and assessment of implant bed conditions. Flap design choices may vary; some clinicians prefer a limited flap while others use full access depending on anatomic considerations. Drilling sequences and osteotomy depth are guided by preoperative planning; primary stability metrics such as insertion torque or implant stability quotient (ISQ) readings are often monitored intraoperatively. These metrics may inform decisions on immediate provisionalization, with teams typically setting conservative thresholds rather than absolute values.
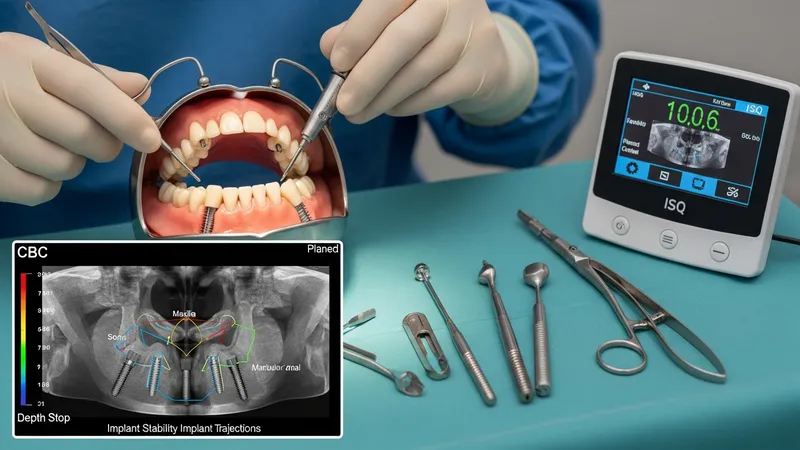
Tilted posterior implant placement requires attention to angulation and emergence relative to the prosthesis. When posterior implants are angled, components and prosthetic abutments are selected to correct prosthetic emergence and to orient screw access favorably. Tilted implants may engage denser cortical bone anteriorly, which can enhance primary stability in some cases. However, clinicians must assess individual anatomy—sinus locations, mandibular canal position, and ridge morphology—to avoid encroachment on critical structures while achieving the planned trajectory.
Computer-guided surgery can be integrated with the operative steps to transfer the planned implant positions to the mouth. Guide-supported osteotomies are typically executed with long drills and guide sleeves, and clinicians often verify guide fit prior to preparation. In freehand placement, planned angles are translated using surgical stents or reference points from the plan. Whichever approach is used, surgeons commonly confirm prosthetic component compatibility intraoperatively and adjust for passive fit to reduce prosthetic stress at the time of loading.
Immediate provisional delivery is a step that often follows implant placement when primary stability thresholds are met. Temporary fixed prostheses are usually designed to control occlusal contacts and to minimize lateral loading during healing. Where immediate loading is not appropriate due to insufficient stability or unfavorable tissue conditions, clinicians may opt for a nonfunctional interim solution and plan definitive restoration after osseointegration. Postoperative protocols commonly include medication management, dietary recommendations, and scheduled follow-up to monitor healing and prosthesis function.