All-on-4 Dental Implants: Understanding The Full-Arch Restoration Procedure
Planning and Assessment for the Full-Arch Four-Implant Approach
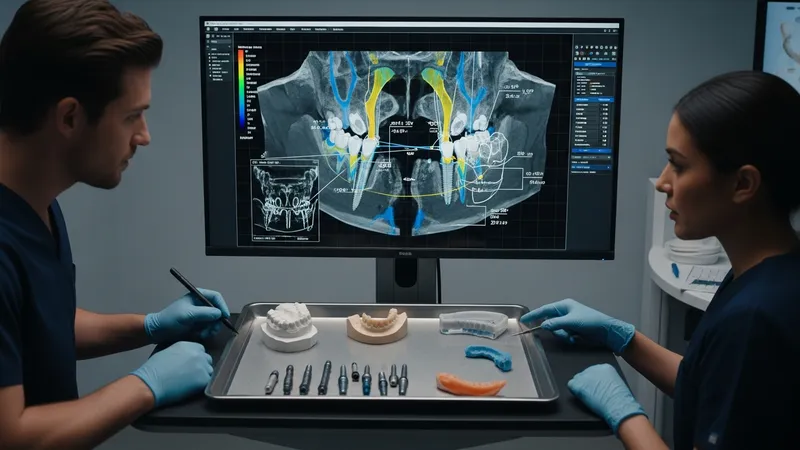
Preoperative assessment for a four-implant full-arch solution typically begins with a comprehensive clinical exam and three-dimensional imaging to evaluate bone volume, sinus anatomy, and neurovascular structures. Digital planning software may be used to simulate implant positions and to design provisional prostheses; this often improves visualization of prosthetic emergence profiles. Case records commonly include study models, photographs, and occlusal analysis. When available, multidisciplinary input from restorative dentists and laboratory technicians may refine the prosthetic plan. These planning steps are considered important for matching implant placement to the intended final restoration while accounting for patient-specific anatomy.
Selection of implant positions usually balances prosthetic needs and bone availability. The anterior implants are often placed axially in denser bone, while posterior implants may be tilted to engage additional anteroposterior bone and to reduce posterior cantilever. Tilted placement can reduce the need for grafting in some jaws, although clinicians typically evaluate sinus proximity and bone angulation carefully. Planning may also consider implant diameter and length choices that correspond to primary stability expectations and prosthetic connector positions used in later prosthesis fabrication.
When computer-guided planning is used, surgical guides can be fabricated to transfer the virtual plan to the surgical field. Guides may be tooth- or mucosa-supported depending on whether teeth remain and on soft tissue conditions. Guided placement may assist in achieving intended angulation and depth, yet clinicians usually allow for intraoperative verification and potential deviations. Accuracy of guided systems can vary and is influenced by imaging quality, guide seating, and the surgical protocol; thus, guided workflows are presented as tools to enhance, not replace, clinical judgment.
Preoperative communication with the dental laboratory regarding provisional design often shapes immediate postoperative expectations. Provisional restorations that are fabricated in advance or milled after planning can be adjusted chairside and are typically designed to control occlusal forces during the initial healing phase. In addition, patient counseling about maintenance needs and realistic timelines for definitive prostheses is commonly discussed. These planning and assessment steps aim to align surgical positioning, provisional prosthetic function, and long-term restorative goals.