AI Medical Coding Platforms: Understanding How Automation Supports Clinical Documentation
Regulatory and coding standards considerations in United States clinical documentation
Automated coding systems in the United States must operate within the framework of national code sets and regulatory guidance. ICD-10-CM is maintained for diagnoses, CPT for procedures and services, and CMS provides payer-specific billing and documentation guidance. Systems that generate code suggestions typically reference current code set versions and implement logic to reflect sequencing rules, modifiers, and documentation requirements. Institutions often align vendor configurations with internal medical record policies and with guidance from CMS or the American Medical Association (AMA) to maintain consistent coding practices.
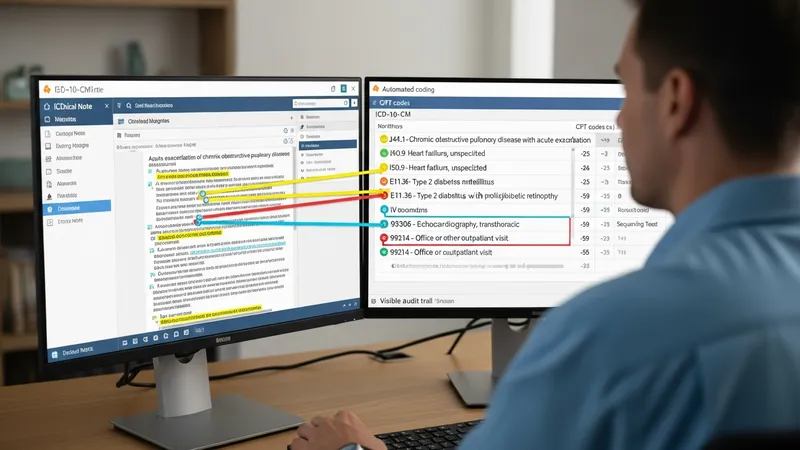
Audit preparedness and documentation support are common regulatory focal points. U.S. healthcare organizations may face internal audits, payer audits, or Medicare program integrity reviews; maintaining accessible audit trails, source text highlights, and reviewer actions can support responses. Automated systems that preserve evidence of reviewer validation and retain linking between suggested codes and source documentation may assist in demonstrating compliance during reviews. Facilities often establish procedures to reconcile automated suggestions with institutional coding policies and legal obligations under applicable U.S. law.
Privacy and data protection requirements under HIPAA guide how PHI is processed and stored. Business Associate Agreements and technical security measures such as encryption, access control, and logging typically accompany deployments. Where cloud or third-party processing is used, contracts and security assessments often address location of data storage, permitted uses, and incident response expectations consistent with U.S. regulatory requirements. These controls are typically considered during vendor selection and contracting stages to ensure alignment with institutional risk frameworks.
Keeping code sets and guidance current is an ongoing activity: annual and periodic updates to ICD-10-CM and CPT, and to payer policy, can affect automated mappings. U.S. organizations often plan for version updates, testing windows, and change management processes so that system behavior remains aligned with current billing rules and documentation standards. Coordination between clinical, coding, compliance, and IT teams typically supports timely updates and reduces risk of mismatches between clinical documentation and coded output.