Cosmetic And Plastic Surgery: Understanding Common Procedures And Outcomes
Types of Procedures in Cosmetic and Plastic Surgery: Categories and Typical Applications
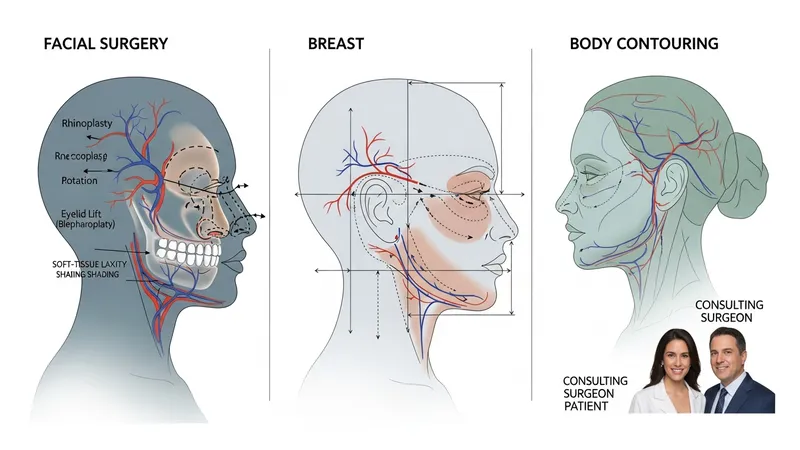
Procedure categories in cosmetic and plastic surgery can be described by anatomical region and by primary goal, such as reconstruction versus aesthetic alteration. Facial procedures may address nasal structure, eyelid position, or soft-tissue laxity, and they often require detailed analysis of facial proportions and skin quality. Breast-related procedures may focus on volume modification, reduction, or reconstruction after tumor removal, each with different technical approaches. Body contouring addresses adipose distribution and redundant skin, frequently following weight loss. Reconstructive cases commonly use grafts or flaps to restore tissue continuity and function. These categories provide a framework for clinicians to select operative strategies aligned with patient-specific factors.
Within each category, technique selection often reflects trade-offs between invasiveness, expected recovery, and potential need for revision. Less invasive options may involve local excisions or office-based procedures with shorter recovery, while complex reconstructions can be staged and require longer convalescence. Scar placement, tissue tension, and vascular supply are technical variables that may influence immediate intraoperative decisions and long-term appearance. Clinicians typically discuss multiple technical options and explain how each may affect healing timelines and secondary procedures, using descriptive comparisons rather than prescriptive recommendations.
Typical applications of these procedure categories vary by patient needs and clinical indications. For example, breast reconstruction following oncologic surgery may prioritise restoration of chest wall contour and symmetry, whereas cosmetic breast modification commonly addresses volume and proportion. Facial procedures can address both function and appearance, such as rhinoplasty for breathing and nasal form. Reconstructive strategies for trauma often require multidisciplinary coordination, including orthopaedics or neurosurgery when deeper structures are involved. Framing procedures by application helps set realistic expectations about stages of care and follow-up requirements.
When considering procedural categories, clinicians frequently reference outcome measures that are relevant to each type. These may include validated patient-reported outcome instruments for breast surgery or scar assessment scales for cutaneous procedures. Objective measures—such as symmetry indices, range-of-motion testing, or photographic comparison—can supplement subjective reports. Such metrics are used to guide follow-up care and to inform decisions about potential secondary procedures, and they tend to be applied as evaluative tools rather than as predictors of individual results.