Neurosurgery: Understanding Common Brain And Spine Procedures
Neurosurgery refers to the clinical field that addresses surgical management of conditions affecting the brain, spinal cord, peripheral nerves, and associated structures. It encompasses procedures intended to diagnose or treat structural, vascular, degenerative, neoplastic, and traumatic conditions of the central nervous system. Practitioners in this field coordinate imaging interpretation, surgical planning, operative execution, and post-procedural follow-up to address anatomic or physiologic disruptions within neural tissues, using a range of open and less-invasive techniques depending on anatomy and clinical context.
Procedural approaches in this area typically involve multidisciplinary input, including neurosurgeons, neuroradiologists, anesthesiologists, and rehabilitation specialists. Preoperative evaluation often focuses on imaging, functional assessment, and risk stratification to match a surgical plan to a patient’s condition. Intraoperative methods and postoperative pathways vary by target (intracranial versus spinal), and the practice generally balances aims of symptom control, structural stabilization, and preservation of neurological function while acknowledging perioperative risks and recovery trajectories.
- Craniotomy for lesion resection — an open skull approach to access intracranial tumors, cysts, or hematomas; often paired with neuronavigation and intraoperative monitoring for anatomic guidance.
- Spinal fusion and stabilization — techniques to stabilize vertebral segments using instrumentation and bone grafting for degenerative, traumatic, or deformity-related instability; approaches may be posterior, anterior, or lateral depending on pathology.
- Endovascular procedures for vascular lesions — catheter-based methods such as coiling or stenting to treat aneurysms or vascular malformations via intravascular access, frequently guided by digital subtraction angiography.
Selection among these and related procedures typically follows a diagnostic framework that may include clinical examination, cross-sectional imaging, and an assessment of functional goals. For example, an intracranial lesion that produces mass effect and progressive symptoms may be considered for resection when imaging and functional mapping indicate a reasonable risk–benefit balance. For spinal conditions, instability or neural compression often informs whether decompression alone or decompression with fusion is contemplated. These determinations frequently involve multidisciplinary case review and patient-centered discussion rather than a single metric.
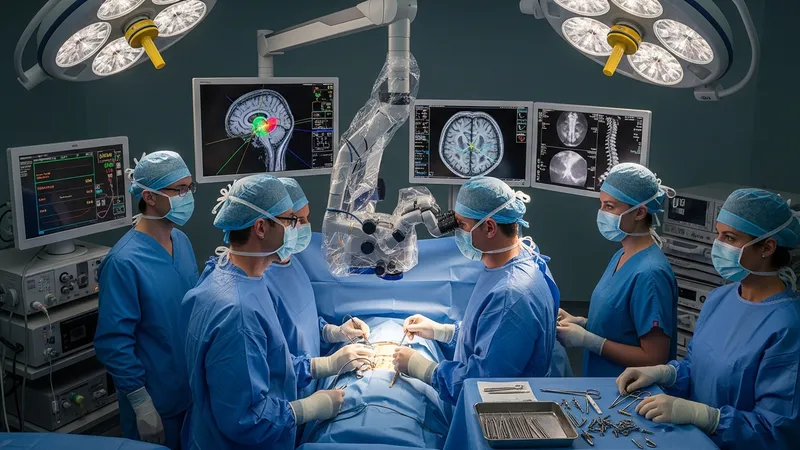
Imaging and intraoperative guidance tools often play a central role in modern neurosurgical practice. High-resolution MRI, CT, and angiographic studies may be used to define anatomy and plan surgical corridors. Intraoperative neuronavigation systems and real-time electrophysiological monitoring can provide additional spatial and functional context, which may influence approach selection and extent of intervention. These adjuncts are intended to support clinical judgment and may help reduce uncertainty during complex procedures.
Operative techniques range from traditional microsurgical exposure to minimally invasive tubular or endoscopic corridors, and from open spinal instrumentation to percutaneous fixation. Each technique carries procedural trade-offs that surgeons and teams typically weigh, such as tissue disruption, visualization, and anticipated recovery course. Endovascular methods may be chosen for vascular lesions when intraluminal access offers a lower anatomical disruption compared with open exposure. Procedural choice often reflects anatomy, underlying pathology, and available expertise.
Post-procedural frameworks commonly integrate early assessment of neurological status, pain management strategies, wound care, and rehabilitation planning. Discharge planning may consider mobility, home support, and the need for outpatient or inpatient rehabilitative services. Outcome measurement is usually multidisciplinary and may include serial imaging, functional scales, and longitudinal follow-up to monitor for complications and to guide rehabilitation intensity. These pathways are adapted to individual clinical contexts rather than standardized in every case.
In summary, the concept covered here addresses surgical interventions for brain and spine conditions through a sequence of evaluation, planning, operative technique, and follow-up. The examples provided illustrate representative procedural categories and the broader considerations that typically inform their use. The next sections examine practical components and considerations in more detail.