VMAT2 Inhibitor Clinical Trials: Overview Of Study Designs And Objectives
Study design types used in VMAT2 inhibitor clinical trials
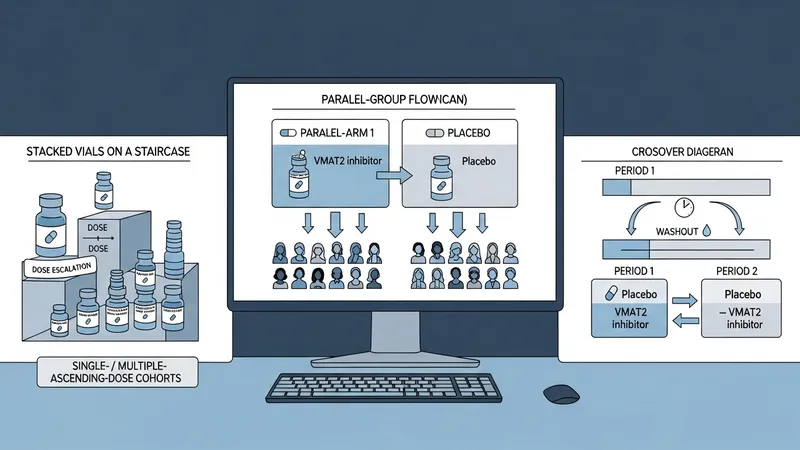
Randomized, placebo-controlled parallel-group trials are commonly used to test efficacy hypotheses for VMAT2‑active compounds in the United States. These designs allocate participants to investigational drug or placebo arms and use prespecified primary endpoints assessed at fixed time points. Crossover designs may be chosen when within-subject comparison reduces variability and when the condition and drug kinetics allow washout periods. Early-phase designs in the US often emphasize single- or multiple-ascending-dose cohorts to define tolerability and pharmacokinetics before larger controlled trials proceed.
Adaptive designs may be considered to improve efficiency; examples include dose-selection adaptations and interim futility monitoring. In the US regulatory context, adaptive elements usually require detailed pre-specification and statistical control of type I error; sponsors often discuss adaptive plans with FDA during development. Open-label extension studies are another common design to collect longer-term safety and tolerability data after controlled phases conclude.
Platform or master-protocol approaches are less common for VMAT2 programs but may be used in broader neuropsychiatric research networks in the United States to evaluate multiple agents under a shared infrastructure. These approaches can standardize outcome measures and reduce redundancy in site activation. Operational considerations for any of these designs include site experience with neuropsychiatric scales, training for raters, and clear procedures for randomization and blinding to maintain data integrity.
When determining a design, sponsors and investigators in the United States typically weigh statistical power, enrollment feasibility, and endpoint reliability. Sample-size assumptions often rely on prior US-based studies or pooled estimates from the literature. Considerations such as expected dropout rates, concomitant medication prevalence, and variability of key outcome measures in US populations are commonly incorporated into protocol planning to ensure interpretable results.