Drug And Alcohol Rehab Centers: Understanding Treatment Options And Care Levels
Care levels and service types in Drug and Alcohol Rehab Centers: Understanding Treatment Options and Care Levels
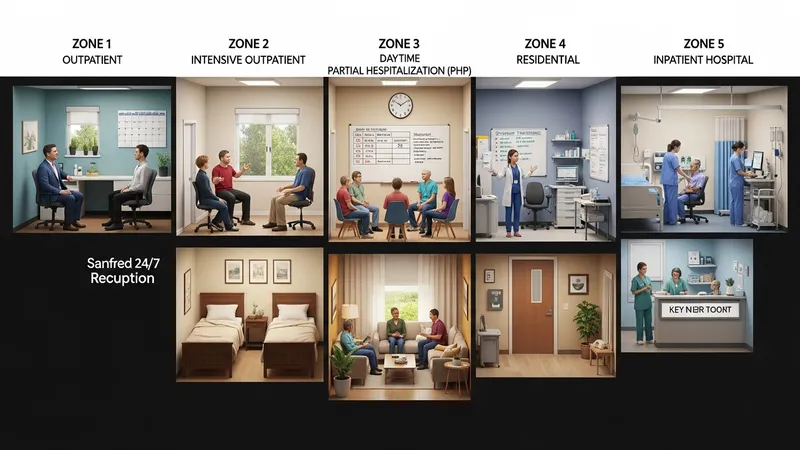
Care levels commonly range from early intervention and outpatient counseling to intensive residential or inpatient services. In the United States, many facilities classify services as outpatient, intensive outpatient (IOP), partial hospitalization (PHP), residential, and inpatient hospital care. Each level typically differs by hours of clinical contact, 24-hour availability, and the degree of medical oversight. Facilities frequently describe the scope of services they provide and whether they follow ASAM placement criteria, which helps clinicians and families compare how a center defines intensity and transition points.
Facility examples in the U.S. illustrate these distinctions: outpatient programs may provide weekly individual therapy and group sessions, IOPs often offer multiple hours per day several days per week, and residential programs provide round‑the‑clock supervision. National directories and state licensing databases commonly list the types of licensure and services available at each center. When reviewing options, it may be helpful to note the typical daily schedule and staff roles associated with each care level to understand how intensity translates into services delivered.
Many centers describe integration of medical evaluation and psychiatric assessment as part of initial placement. For people with co-occurring mental health conditions, combined behavioral health services may be offered on-site or via formal referral agreements. The presence of credentialed medical personnel or formal partnerships with hospitals can influence whether a facility provides medically managed detoxification or refers out to hospital settings when higher levels of medical care are required.
Data sources such as the Substance Abuse and Mental Health Services Administration (SAMHSA) and state health departments provide listings and program descriptions that reflect observed patterns across the U.S. These resources may show that program availability and commonly used care models differ by region; rural areas, for example, often rely more on outpatient and telehealth services whereas urban regions may have greater access to residential beds. Such patterns inform how systems plan and allocate resources.