Deutetrabenazine Medication: Overview Of Uses, Mechanism, And Key Considerations
Clinical mechanism and neurotransmitter interactions for Austedo
The principal pharmacologic action of this class involves inhibition of the vesicular monoamine transporter type 2 (VMAT2), which plays a central role in sequestering monoamines into synaptic vesicles. By reducing vesicular uptake, the pool of transmitter available for stimulus-evoked release may be diminished. Dopamine modulation is often the primary focus in movement-disorder contexts, but effects on other monoamines can contribute to clinical and adverse effects. Preclinical and clinical pharmacology reports typically describe concentration-dependent effects and note that central nervous system outcomes arise from altered synaptic monoamine dynamics rather than direct receptor antagonism.
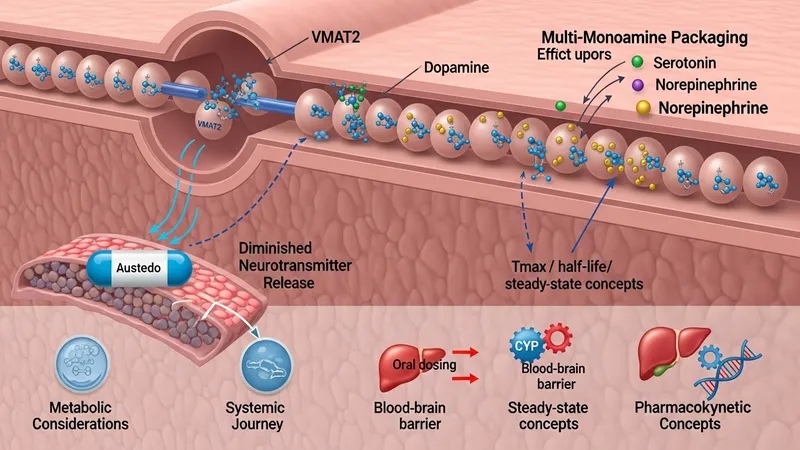
Pharmacokinetic characteristics such as oral bioavailability, time to peak plasma concentration, and half-life influence dosing schedules and steady-state attainment. Some agents in this class have been chemically modified to slow metabolic clearance, which can change exposure variability and dosing frequency. Metabolism is commonly hepatic, involving pathways that may be sensitive to genetic variation and interactions with enzyme inhibitors or inducers. These factors are often documented in regulatory labeling and clinical pharmacology reviews as considerations for clinicians and pharmacologists.
Neurotransmitter interactions relevant to clinical effects include secondary influences on serotonergic and noradrenergic signaling that may occur when vesicular monoamine storage is altered. Such interactions may underlie some psychiatric or autonomic adverse effects observed in trials. Because monoamine homeostasis is complex, investigators often monitor behavioral and affective symptoms in clinical studies and post-marketing settings to detect signals that might warrant additional study or label updates.
Translational research into transporter-targeting agents often includes neuroimaging, neurotransmitter metabolite assays, and electrophysiologic measures to better define mechanism–outcome relationships. These methods can illustrate how modulation of vesicular transport changes circuit-level activity in motor control regions. Readers should note that mechanistic understanding evolves as new studies refine relationships between transporter inhibition, neurotransmitter availability, and clinical manifestations.